Science for the Tech Diver – NEDU Study
Since I am a physiologist and a technical diver at the same time, I try to improve my knowledge of hyperbaric physiology by reading the original scientific literature in the field. I hope that my thoughts on these topics, which I am sharing here, are useful to my fellow divers. Maybe I can also help some divers to get a better hold of these topics by presenting pre-digested summaries of these scientific papers here. A lot of science is actually very common-sensical and unfortunately made hard to understand by the use of complicated lingo. Just stripping the actual content of this lingo, and adding a bit of background, can go a long way in making scientific insights more comprehensible.
A recent paper by hyperbaric researchers from the Navy Experimental Diving Unit, Doolette, Gerth and Gault, has caused quite some discussion in the technical diving community. The study is titled “Redistribution of decompression stop time from shallow to deep stops increases incidence of decompression sickness in air decompression dives”.
Basically, they take volunteer Navy divers, and put them in a “wet pot” – a deco chamber filled with water. This allows them to control the conditions much more closely than when doing ocean dives. Keeping the divers submerged is more realistic than having them sit in a dry chamber at the same pressures. While submerged the divers were made to pedal on stationary bikes. After resurfacing they were checked for DCS, and their venous bubbles were checked by ultrasound.

The study analyzes 390 dives, a really large number, about half with deep stop and half with shallow stop profiles. As far as I can judge, the authors did a good job with the study design and analysis.
The amount of decompression incidents was higher in the case of the dives conducted with deep stops, and the amount of bubbles detected by ultrasound was higher. At the end of the paper, the authors compare the supersaturation in fast and slow tissues with profiles with more or less deep stops. This part is theoretical – comparing the effects of diving schedules based on calculations of tissue pressure – ambient pressure gradients. Here they conclude that deep stops help the fast tissues, but hurt the slow tissues when it comes to supersaturation load.
I think we need to keep a few things apart:
– gas content-based algorithms versus bubble based algorithms
– deep stops versus no deep stops
– the experimental part and the theoretical part of this study. In brief: They compare models with models. We don’t know if all the relevant components of decompression in tissues are included in the model they compare the schedules against. Let’s take this part with a grain of salt.
The decompression algorithms used in the study are not exactly what the tech divers I know would use, but they are still a gas content-based algorithm and a bubble based algorithm. The authors explain that “In the Thalmann Algorithm, when a compartment is supersaturated, compartment gas kinetics may switch from exponential to linear, slowing gas washout and prolonging decompression stop times.”. An interesting feature of this algorithm, I assume it’s meant to model tissue damage which slows down gas washout.
My main issue I have with the applicability of this study is that test divers were made to pedal at stationary bicycles with a power of 130 Watts. That’s a lot – some of the divers couldn’t do it, and the resistance had to be reduced. And we are not talking about middle aged vacation divers who had to have the work-load reduced, but about fit Navy dudes, with an average age of 37 and an average body fat percentage of 15 (that’s quite low). This is a significantly higher rate of physical exertion than what’s usual during civilian tech dives. When I dive, I hover, meditate and fish-watch, and move as little as I can. The study might have explored a different parameter regime that what is relevant to tech divers like me and my mates. The divers in the study might have gone into anaerobic (not-oxygen consuming) metabolism due to the high exercise intensity. We can only speculate how that affects decompression. Lactate buildup in the muscles, and a resulting change in tissue acidity could affect the gas dynamics of the body (see the Bohr Effect) in a way significant for decompression.
Also the authors state that “Whereas divers were thermally comfortable early in the dive, they generally became cold while at rest during the decompression.” – this is also not how I conduct my decompression dives. In the Philippines I dive with a rash guard only, since the water rarely drops below 26C. I never feel any cold discomfort. If you do, then you should wear more neoprene (or eat more ice cream).
Maybe that heavy exertion was necessary to make sure enough cases of (slight) DCS occur to make the differences between the bubble and gas content model significant? Still, the qualitative difference persists. Maybe this situation (heavy exertion at depth, being cold) is typical for military diving? I don’t know – I have several friends who are/were in the US Navy, maybe they can shed some light on this question. Does the enemy try to get away in 170 fsw by swimming extra fast? Then the enemy is going to get bent, too!
In any case, the situation experimentally tested during this study seems to be significantly different from what is encountered during civilian technical diving how I know it. In my opinion it is premature to modify time-tested deco protocols for civilian tech divers in warm water based on this study.
I want to add a fundamental thought about models at this point. I like bubble models better because they include more known physics about the processes we are interested in. In science, a discrepancy between “black box models” and “mechanistic models” often comes up. If I observe any type of process in nature, and that could be decompression sickness as a function of deco profiles, or heart attacks as a function of body fat content, I can simply fit a curve to it. I can find a simple and efficient mathematical description which gives me the chance of DCS, or of a heart attack, given the dive profile or the body fat content. I don’t need to understand anything about the mechanisms which cause DCS or heart attacks – I just summarize statistics in an (preferably short) equation.
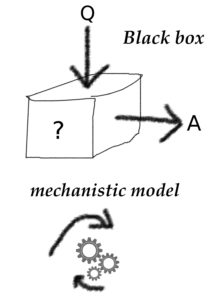
In contrast, I can make a mechanistic model which includes as much detail about the problem at hand which I have reliable knowledge about. In the case of DCS, where bubbles cause damage in the body, I will include as much about bubbles as I can. The bubble models used in diving have included quite a bit of detail about the formation and growth of bubbles.
A mechanistic model is not necessary better than a black box model. If the curve-fitting of the black box model is done very well, and the parameters of the mechanistic model are off, then the black box model might outperform the more realistic mechanistic model. The type of model is one thing – to me a mechanistic model which explains something about the innards of the process I am interested in is superior. The quality of the model is another thing – a mechanistic model might be poorly implemented (with wrong parameters).
There is a gradient between black-box and mechanistic models. The gas content-based algorithms are not completely agnostic about gas in different tissues. They include a simple model of diffusion between the breathing gas and the body. They also include different compartments which are equivalent to tissues of the body (though only very roughly). The bubble models include much more detail about the physics of decompression. Any new insights about the mechanisms of bubble formation, transport and removal can be integrated more easily into bubble models.
So, in my mind the question should not be “gas content-based algorithm or bubble based algorithm”, but how to improve the more realistic algorithm (the bubble based algorithm).
There has been considerable discussion of this study and it’s consequences on several online boards, with input by very qualified divers. This and this are two threads on rebreatherworld dealing with the topic. This discussion has been going on for a while, I hope my contribution is still useful.